Abstract
Rationale: Pulmonary embolism (PE) is a major cause of morbidity and mortality. Using D-dimer thresholds to rule out PE in high-risk individuals is debated.
Methods: We reviewed 1206 consecutive CTPAs to identify high-risk cases. To account for the absence of information on ?PE is the most likely diagnosis?, modified Wells scores were calculated in conservative and liberal estimates (excluding or including +3 for ?most likely diagnosis? respectively) in both the original and ?2?level? versions of the score. Only data from CTPAs accompanied by D-dimers measured within the prior 24 hours were included. The performance of normal (<500pg/mL) and age-adjusted D-dimer (a-aD) thresholds at ruling out PE in high-risk patients was then retrospectively assessed.
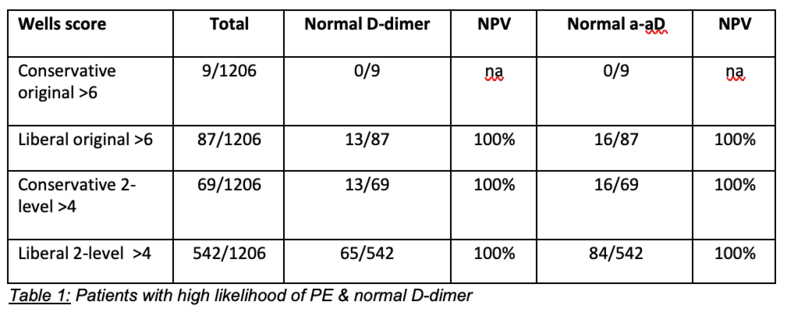
Results: Overall PE was identified in 188/1206 patients (15.6%). By the most conservative estimation of Wells (Score >6, no points assigned for ?most likely diagnosis") only 9 individuals were deemed high-risk and none had normal D-dimers or a-aD. In all other estimations of high-risk Wells score, normal and a-aD effectively predicted absence of PE (negative predictive value 100%). Results are summarised in table 1.
Conclusion: Normal D-dimer and age-adjusted D-dimer may be effective at predicting absence of PE in cases deemed high-risk by clinical decision rules such as Wells. Prospective studies will be needed to validate these findings.