Abstract
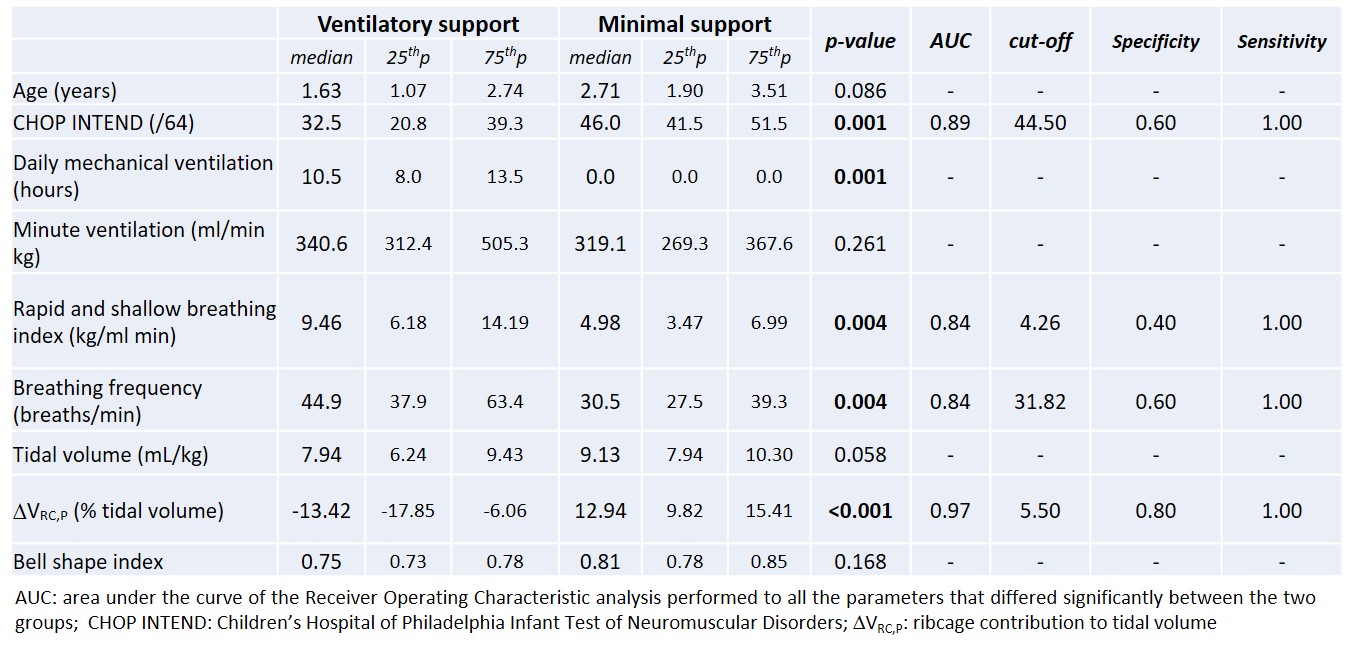
SMA1 is a severe neuromuscular disease resulting in severe muscle wasting. Although motor function has dramatically improved thanks to medications, the respiratory function still remains a critical aspect. The indication to start ventilatory support in SMA is based on clinical rather than quantitative assessments, because volitional and invasive tests are not feasible for infants. We aimed to investigate if the analysis of spontaneous breathing at rest in supine position (assessed through OEP) might predict the need for respiratory support (assessed through the GSR score, a clinical respiratory score based on airway clearance and non-invasive ventilation requirements) in 27 SMA1 children under nusinersen treatment. Two groups were identified: 10 children requiring minimal respiratory support (GSR?15) and 17 with higher requirements (GSR>15). The latter had lower motor function scores, and rapid, shallow and paradoxical breathing indicated by the negative ribcage contribution, which was the strongest predictor of maximum respiratory support request. Its positive cut-off point indicated that respiratory support must be initiated when a residual action of ribcage muscles is still present, well before the onset of paradoxical thoracic breathing (Table). Spontaneous breathing can predict the need for ventilatory support without requiring cooperation and/or invasive tests in SMA1 infants.