Abstract
Background: Clinical diagnosis of respiratory disease is largely reliant on the reporting of symptoms, in particular dyspnoea and cough. Limited data are available about geographic and socio-cultural differences in respiratory symptom reporting.
Aims: To estimate the prevalence of self-reported dyspnoea and chronic cough across 41 sites of the BOLD study.
Methods: In the BOLD cross-sectional survey, dyspoea was assessed in adults (>40 years) using the modified Medical Research Council (mMRC) dyspnoea scale. Dyspnoea was defined as a mMRC ? 2. Chronic cough (CC) was defined as presence of cough during most days for at least 3 months each year.
Results: We included 25,806 participants in this study. Prevalence estimates of dyspnoea and chronic cough are summarised in figure 1. Most sites show prevalence estimates for both dyspnoea and CC of <20%. Sub-Saharan countries show the lowest prevalence of CC and dyspnoea. Of note is the high prevalence of dyspnoea in 8 sites without increased prevalence of CC. No geographical clustering of these sites could be identified.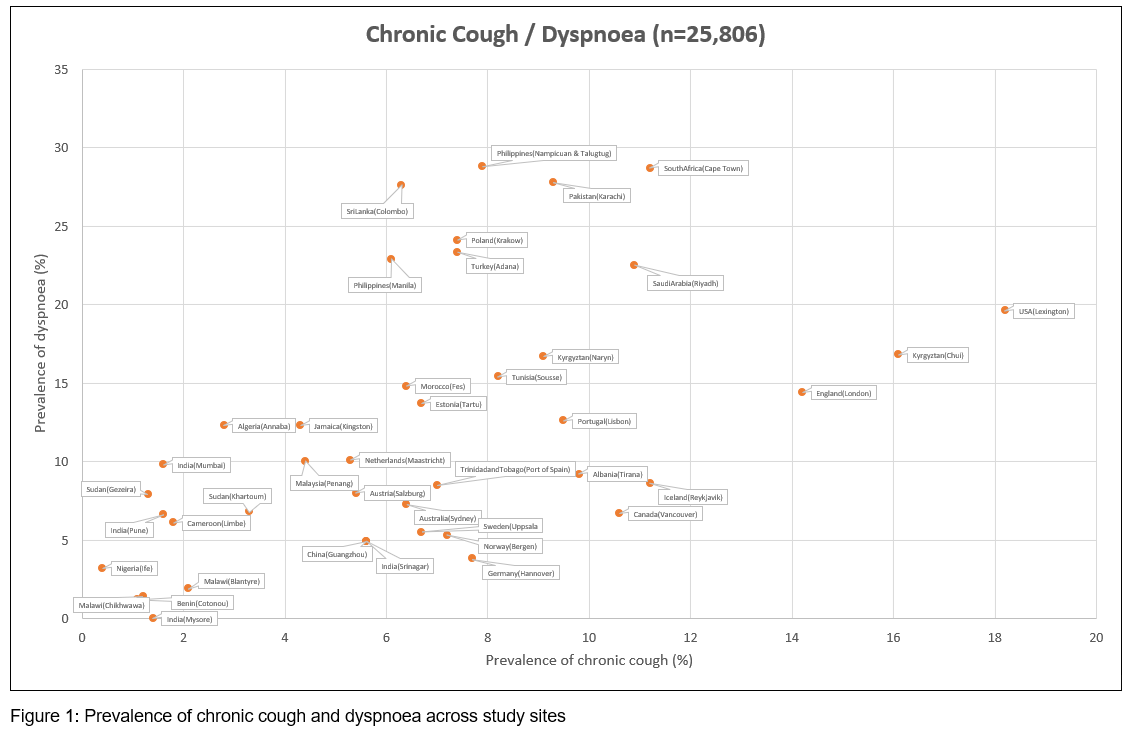
Conclusion: In terms of clinical awareness of respiratory symptoms, our data indicate the need to consider site-specific information on symptoms reporting as possibly modified by socio-cultural and environmental determinants. Further studies are needed to examine the link between variation in symptom reporting and other parameters such as spirometry.