Abstract
Background: Completing PR is positively associated with survival1, but whether due to a direct effect or unmeasured confounding is unknown. We aimed to investigate the association between survival and achieving the MID in walking distance (WD) following PR.
Methods: PR services across England and Wales provided data to a national audit programme (NACAP) for consenting patients assessed between Jan ? April 2015. Mortality data from national records until Jan 2017 were used. Cox proportional hazard regression, unadjusted and adjusted for multiple covariates, was performed comparing time to death between achieving the MID or not using 25m for the six-minute WD (6MWD) and 35m for the incremental shuttle WD (ISWD). Missing data were imputed.
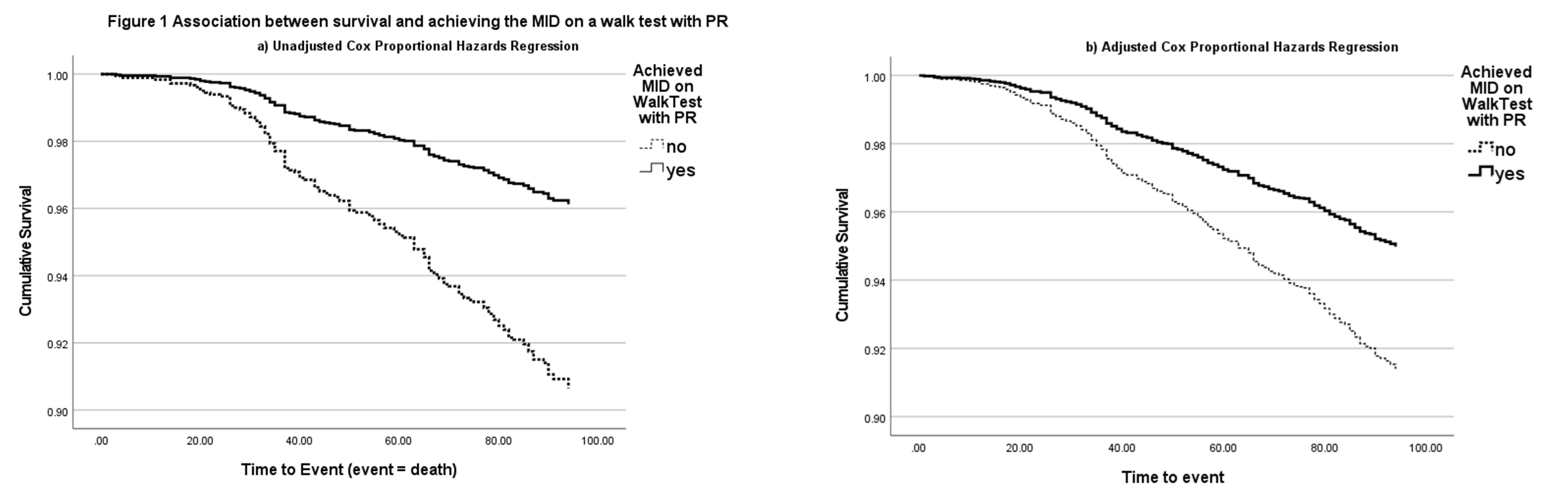
Results: Walk tests before and after PR were completed by 3721/4159 (89%) patients (55% male, mean age 70.3 (SD 8.8) years, FEV1 1.38 (0.58)L). Mean (SE) change in ISWD and 6MWD was 63 (2)m and 57 (2)m, respectively. 273 patients (7.3%) died by Jan 2017. Unadjusted and adjusted mortality rates were lower for those achieving the MID in either walk test, HR 95%CI 0.40 (0.29?0.56) and HR 0.57 (0.45?0.72), respectively (Figure 1), p<0.001.
Conclusion: In this large, real-life dataset improved walking distance more than the MID following PR is positively associated with survival potentially indicating a direct effect of completing PR.
1ERJ2019,54:OA3577