Abstract
Background: Previous studies in pediatric asthma demonstrated proximal and distal inflammatory patterns were related to their clinical manifestations, but it remains unknown in adult asthma.
Methods: We recruited 233 stable asthmatic patients (165 females; mean age 52.7±15.0 years-old; mean daily dose of inhaled corticosteroids 662±354 ?g/day [fluticasone equivalent]) who completed Asthma Control Test, blood tests, the fraction of exhaled nitric oxide (FeNO), and spirometry. FeNO was measured at different expiratory flows to calculate J?awNO (maximum airway NO flux) and CANO (alveolar concentration of NO). Patients were categorized as type I (normal J?awNO and CANO), type II (elevated J?awNO and normal CANO), type III (elevated J?awNO and CANO), and type IV (normal J?awNO and elevated CANO) by the cut-off points with 1470 pl/s and 4.5 ppb, respectively (Figure).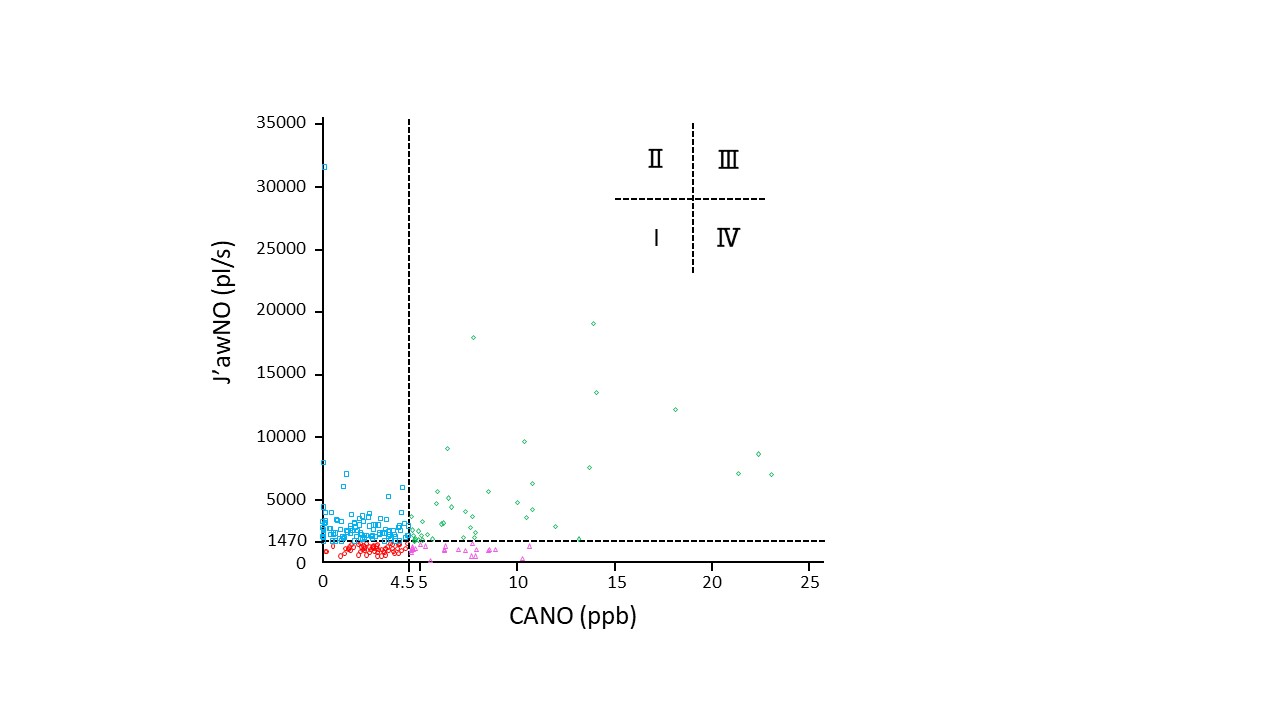
Results: The average ACT scores were significantly low in type ?. Additionally, the proportion of patients who received treatment step 4 and 5 according to the Global Initiative for Asthma guideline and who needed admission due to asthma exacerbations were significantly high in type IV. In type III, impaired pulmonary function and increased blood eosinophil counts were observed.
Conclusions: The classification categorized by proximal and distal airway inflammation may reflect distinct clinical features in patients with adult stable asthma.