Abstract
In Covid-19, PaO2/FiO2 ratio (PF) predicts mortality in patients with acute respiratory failure (ARF) treated with invasive or non-invasive ventilatory support.
Aim of this study was to evaluate if PF measured at emergency room (ER) admission predicts mortality in patients with Covid-19 ARF breathing room air or supplemental oxygen.
We enrolled 433 patients (215 male; 218 female) with Covid-19 pneumonia and ARF (PaO2<60mmHg and PF<300). PF was measured at ER (T0), at ward admission (T1) and at ARF nadir (T2). To define PF accuracy to predict mortality we used receiver-operating characteristic (ROC) curve.
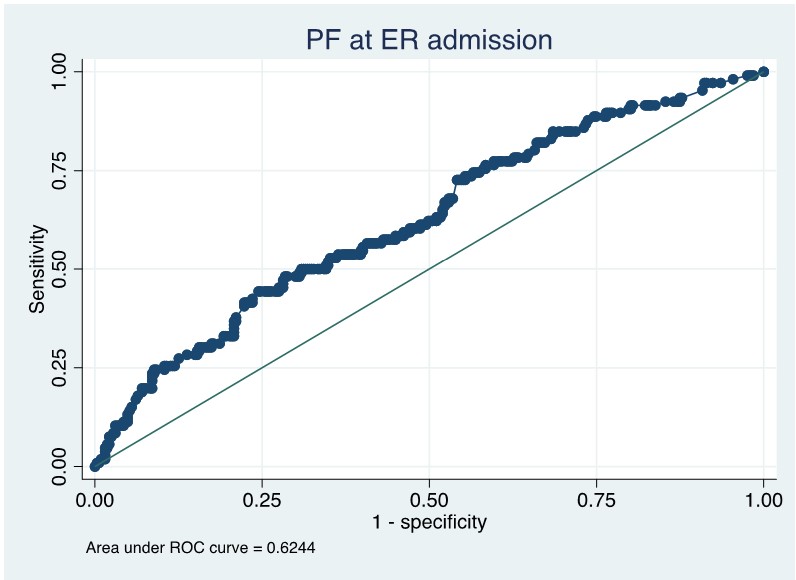
At T0, PF median value was 174 (109-257); 37.2% of patients were in room air, 62.8% were on supplemental oxygen. At T1, PF median value was 152 (116-196); almost all patients received positive pressure support (35.2%) or high flow oxygen therapy (34.9%). At T2, PF median value was 149 (108-198); 57.2% of patients were on positive pressure support. Mortality at 28-day was 24.5%. Considering 28-day mortality, area under the ROC curve (AUROC) values were 0.6244 at T0 [Fig.1], 0.6186 at T1 and 0.6813 at T2.
PF at ER is a good predictor of 28-day mortality in patients with Covid-19 ARF breathing room air or supplemental oxygen. Of notice, this is the first large retrospective study demonstrating the prognostic role of PF in very early stage of Covid-19.