Abstract
Background: DLCO and KCO are markers derived from the carbon monoxide (CO) gas-transfer test. There is need for more precise understanding of how lung structure alters these markers, mainly in cases of ventilation-perfusion (V/Q) abnormality.
Aims: Development of a math model to enhance understanding of structure-function (S-F) effects on
DLCO&KCO.
Methods: We developed a 4-compartment V/Q model of the test (Fig 1), using lung capacity (TLC), alveolar volume (Va), pulmonary blood volume (PV), relative lobar V-Q distribution, and diffusivity (D=28.05mL/min/mmHg) (PMID: 3154613) based on a healthy DLCO value in normal diffusion with a PV=0.25L as inputs. We used reference values from published literature to understand how DLCO&KCO outputs change in lung disease.
Results: Model DLCO&KCO values were concordant with reported changes post pneumonectomy (63% DLCO, 106% KCO), pulmonary hypertension (57%,57%; from ~30% decrease in PV & D) and asthma (100%,119%; from 30% decrease in TLC:Va ratio) (PMID: 22538804).
Conclusions: The model produced consistent estimates of DLCO&KCO changes in disease and may provide valuable S-F insights. We aim to further compartmentalise the model using patient-specific imaging biomarkers to generate additional insights.
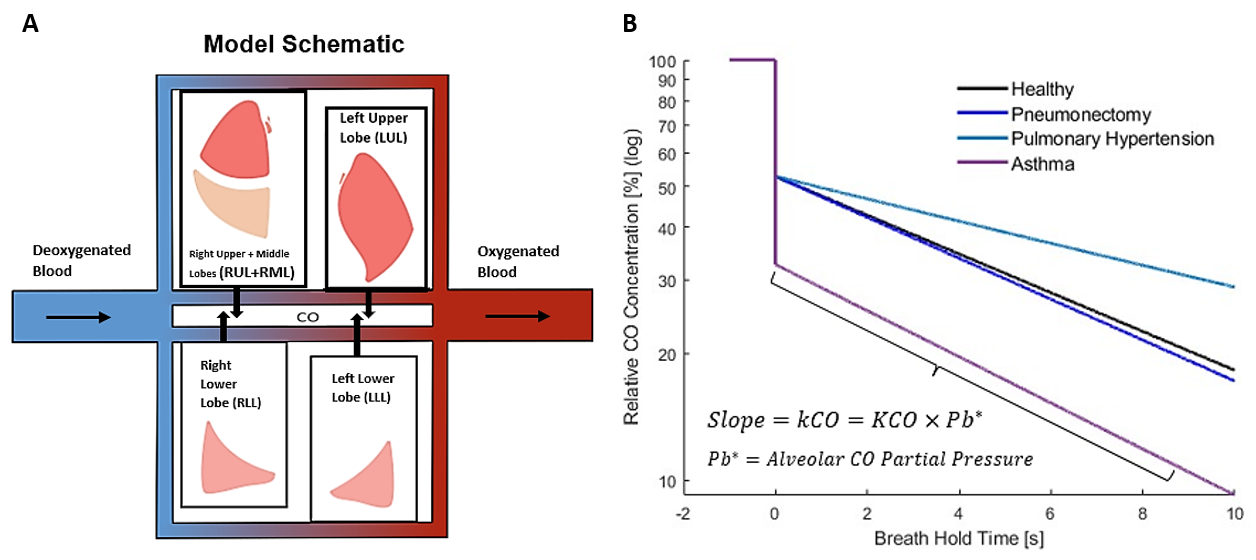
Fig 1 ? Model schematic. A, Blood flows from the heart past 4 compartments, as CO diffuses across the alveolar-capillary membrane. B, CO concentrations over 10s for 4 physiologic states.