Abstract
Background: Increasing severity of COPD is associated with increased risk of mortality and hospitalisation.
Aim: To investigate whether treatment intensity level (TIL) can be used as proxy for disease severity in COPD.
Methods: Patients with COPD alive 1 January 2017 were identified in the period 2001?16 in Danish nationwide registries. Patients were stratified into seven TIL (no use, short-term, mono, dual, triple therapy, oral corticosteroid (OCS), and long-term oxygen (LTOT)). We assessed the inverse propensity-adjusted five-year mortality and the composite of mortality and hospitalization after index date.
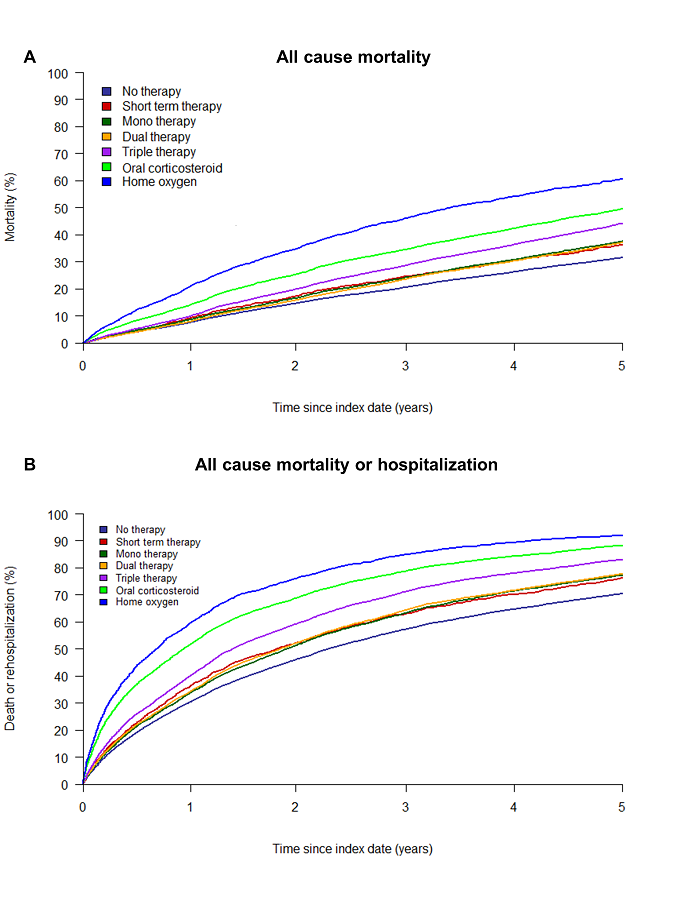
Results: We identified 53,803 patients with COPD (median age: 72 years [64-80], 48% men). Increasing TIL was associated with increasing 5-year mortality and mortality or hospitalization (Figure 1). No significant differences were seen for short-term, mono, and dual therapy use. For triple therapy, OCS, and LTOT a significant consecutive increase was shown (Mortality HR (95% CI): triple therapy 1.52 (1.46-1.58), OCS 1.83 (1.75-1.91), LTOT 2.55 (2.40-2.72)).
Conclusion: Increasing TIL was associated with five-year mortality and risk of hospitalization. TIL may be used as a proxy for COPD severity in future studies.
Figure 1: Inverse probability of treatment weighted Kaplan-Meier functions of the association between treatment intensity level and mortality (A) and mortality or hospitalization (B) in COPD.