Abstract
Background
Premature ventricular complexes (PVC) are common in patients with heart failure with reduced ejection fraction (HFrEF) and central sleep apnoea (CSA). However, it is unclear, if the burden of PVC rises from the 1st to the 4th quarter (Q1, Q4) of the night and if these changes are associated with changes in respiratory parameters (apnoea-hypopnea-index [AHI], loop gain) reflecting the deterioration of cardiac function.
Methods
This subanalysis of the SERVE-HF Major Substudy included patients with left ventricular ejection fraction ?45% (LVEF) and CSA (AHI>15/h) with ?5 stable cycles of periodic breathing in Q1 and Q4 in sleep stage N2 and >30 PVC/h. Patients were stratified into an increased and decreased collective of PVC (PVC+; PVC?) overnight.
Results
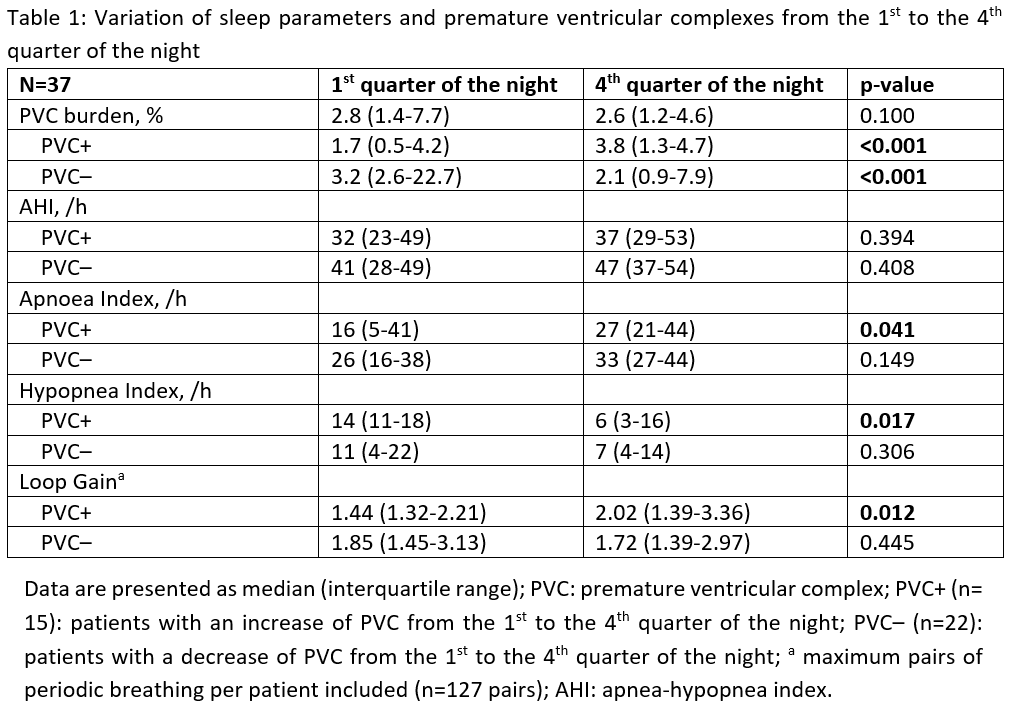
Of 312 patients, 37 (68 years, LVEF 31%, NYHA III 81%) fulfilled the selection criteria. In the total population, the median PVC burden was similar in Q1 and Q4 of the night (2.8% (1.4-7.7)) vs. 2.6% (1.2-4.6), p=0.100). In contrast to patients with PVC?, patients with PVC+ had an increase in loop gain and AI from Q1 to Q4 of the night (table 1). HI decreased significantly in PVC+.
Conclusion
In patients with CSA and HFrEF, PVC burden is similar in the 1st and 4th quarter of the night. However, in patients with an overnight increase of PVC, the increase in loop gain and the shift of hypopneas to apnoeas may reflect a worsening of cardiac function overnight.