Abstract
Aim
The grading of obstructive sleep apnoea (OSA) using the apnoea hypopnoea index (AHI) is increasingly insufficient to guide treatment, although AHI ? 30 has been proven to show worse prognosis. The Baveno OSA classification (2021) incorporates symptoms and physiological consequences. We hypothesize that adding cardiovascular disease (CVD) risk and an estimation of hypoxic burden (HB) using sleep study parameters will facilitate the management of OSA patients.
Method
13916 cases from the European Sleep Apnea Database (ESADA) were retrospectively analysed. HB was estimated using time spent with an oxygen saturation under 90% (T90). Risk stratification of patients was based on SCORE2 for apparently healthy persons and the European Society of Cardiology (ESC) guidelines for those with established CVD, identifying low to moderate, high and very high risk categories.
Results
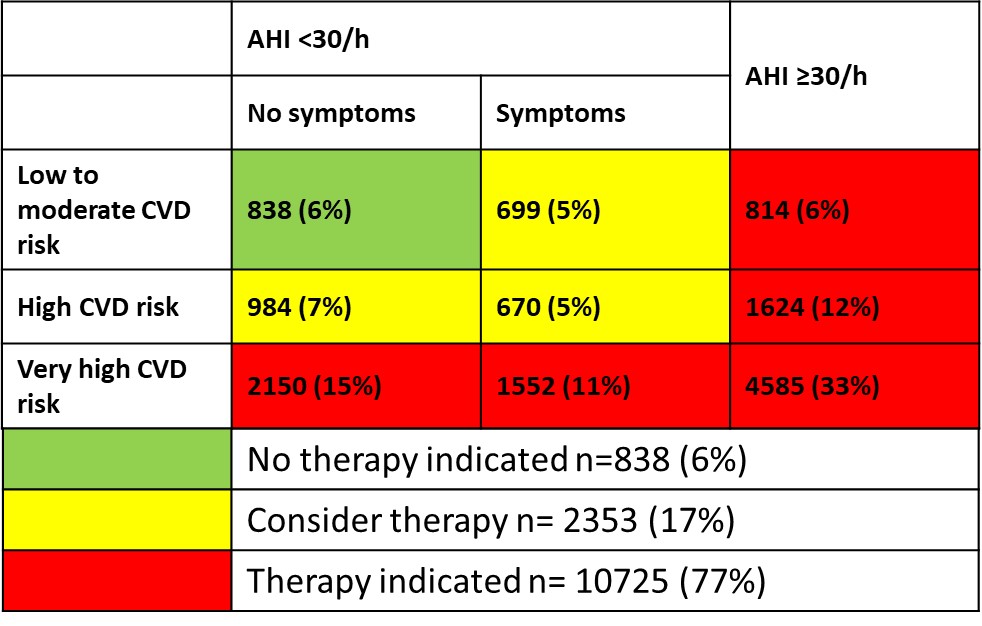
Figure 1 shows the distribution of the cases based on our OSA classification. The median T90 (14.2 min) used as a cut-off identified a similar cohort of patients as AHI </?30/h. T90 vs. AHI showed moderate correlation (r=0.502 , p<0.001), thus AHI was used. A traffic light system guides therapy indication.
Discussion
A high proportion of ESADA patients have AHI >30. The study is limited by the lack of data in ESADA needed for differentiation between high and very high CVD risk, resulting in a high proportion of patients in the definite therapy group.