Abstract
Introduction
Lactate dehydrogenase (LDH), a widely available biomarker, is associated with disease severity in IPF. However, LDH is unspecific, and these associations could be caused by factors unrelated to lung fibrosis.
Ojective
To assess the association between LDH and lung fibrosis on HRCT.
Methods
We selected IPF patients with HRCT scans at the time of diagnosis and after two years. The scans were scored by two experienced thoracic radiologists using a standardized form and blinded to patient data, each-others scores and the time of scan. The extent of reticulation, traction bronchiectasis and honeycombing was combined into a composite quantitative fibrosis score.
Results
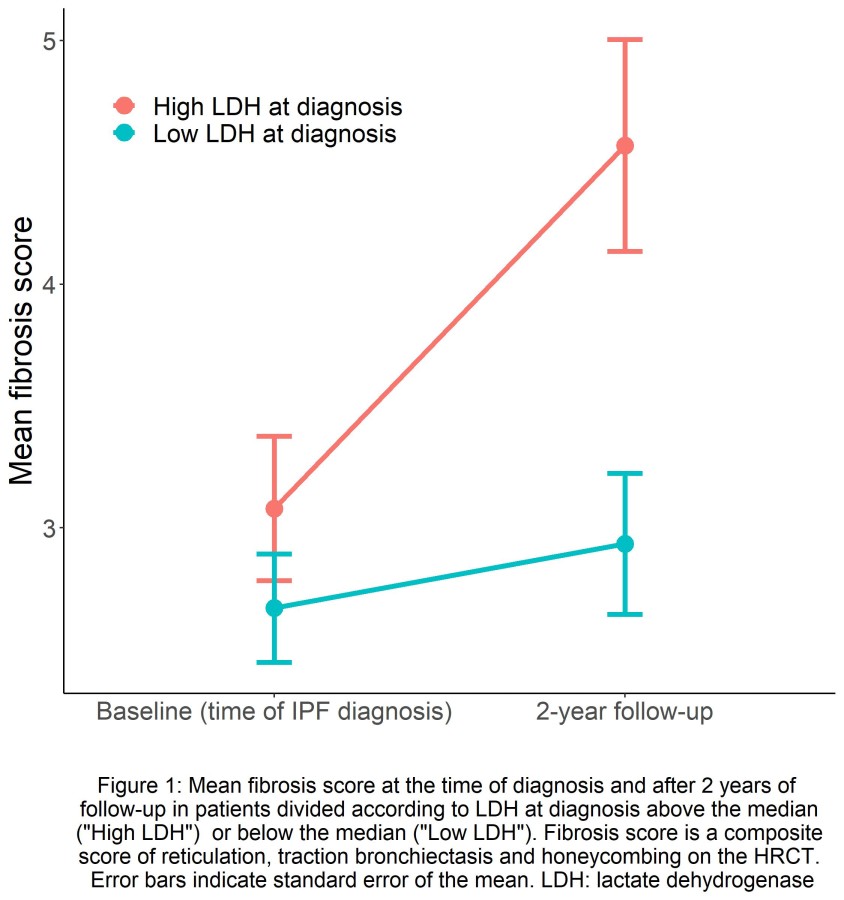
The 66 included patients were divided into a ?high LDH? and a ?low LDH? group around the baseline median LDH.
During the first two years after the IPF diagnosis, the mean fibrosis score increased in the ?high LDH? group from 3.08 to 4.57 (p-value for change: 0.0065). No significant change in fibrosis score was observed in the ?low LDH? group (2.67 to 2.93, p-value: 0.47). This association was confirmed by multiple linear regression analysis adjusted for age, sex and antifibrotic treatment received during follow-up (p=0.004).
Conclusions
LDH, measured at the time of IPF diagnosis, can predict subsequent increase in fibrosis on the HRCT scan. The known association between LDH and disease severity in IPF is therefore likely to be directly related to progression of lung fibrosis.