Abstract
Transcutaneous pCO2 (tcpCO2) device provides a noninvasive estimation of pCO2, whose increased levels in arterial blood define alveolar hypoventilation.
CPAP could be the first-line treatment for OHS patients with concomitant severe OSA whereas noninvasive ventilation (NIV) should be considered as first line therapy for OHS patients with no OSA or milder forms of OSA. Thus, gas exchange should be monitored for the first 2-3 months after initiating PAP therapy.
OBJECTIVES
To assess efficacy of tpCO2 as a tool of control improvement in gas exchange after 3 months of positive airway pressure in patients diagnosed of severe OAS and/or OHS.
METHODS
Severe OSA/SHO patients treated with CPAP/BIPAP/AVAPS. After three months of initiating therapy they were clinical controlled, devices parameters monitored. During wakefulness a 20 minutes transcutaneous capnography was performed. Therapies were assessed depending on the results.
RESULTS
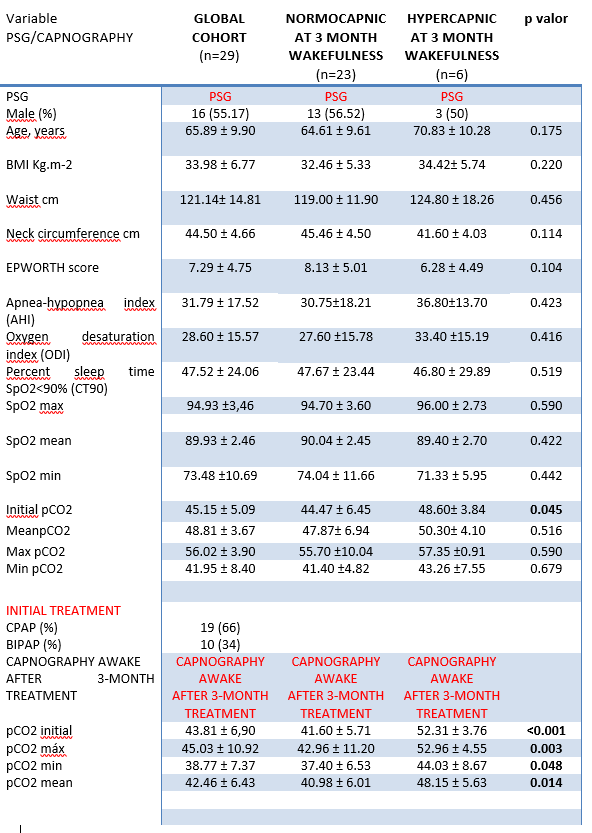
We studied 29 patients. There were no statistical differences obtained during diagnostic PSG. Initially 19 (66%) patients were titrated with CPAP: 10 cm H2O ±1.16 and 10 (34%) BIPAP: IPAP 16.44±2.78 and EPAP 8.25±1.48.
According with results of wakefulness capnography 3 CPAP are switched into BIPAP; 1 BIPAP into AVAPS and 2 BIPAP increase pressure support.
CONCLUSION
Transcutaneous capnography is a noninvasive method to monitor pCO2 during PSG in the diagnosis of alveolar hypoventilation and as a guide to titration.