Abstract
Background: The frequency of community acquired respiratory bacterial coinfection upon hospital admission in COVID-19 patients has been reported to be <4%, but almost three-quarters of patients received antibiotics.
Aim: To investigate whether procalcitonin(PCT) upon admission could be used to identify bacterial coinfection in patients with COVID-19 pneumonia.
Methods: Multicenter, observational cohort study including consecutive COVID-19 patients admitted to 55 Spanish ICUs. Primary outcome was to explore whether PCT levels upon hospital admission could predict bacterial coinfection. Secondary outcome was to evaluate the association of PCT with 30-day mortality.
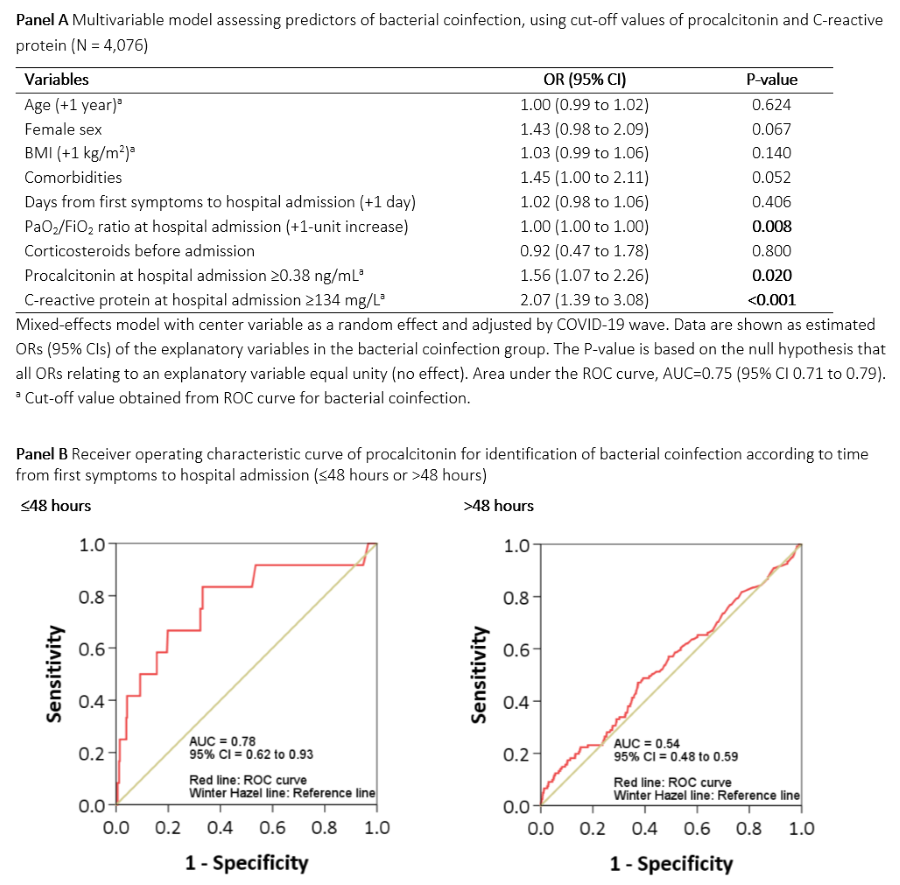
Results: 4,076 patients were included, 133(3%) of whom presented a bacterial coinfection. PCT at hospital admission was independently associated with bacterial coinfection, particularly PCT?0.38 ng/ml(Fig1, A) and with higher 30-day mortality(HR 1.25, 95% CI 1.09-1.45, p=0.002). In the first 48 hours since symptoms onset, bacterial coinfection patients had higher PCT(PCT p=0.001); PCT performed better at the ROC curve analysis(Fig1, B) and values of PCT?0.44 had higher sensitivity and negative predictive value.
Conclusion: PCT levels upon admission are independently associated with bacterial coinfection among patients with COVID-19 pneumonia. PCT<0.44 can be a valuable indicator of the absence of bacterial coinfection within the first 48 hours after symptoms onset.