Abstract
The chester step test (CST) might be an alternative to 6-minute walk test (6MWT) to assess functional capacity, especially in space-constraint settings. We explored its ability in distinguishing people with interstitial lung disease (ILD) with/without functional impairment and at low/high risk of mortality, according to the 6MWT.
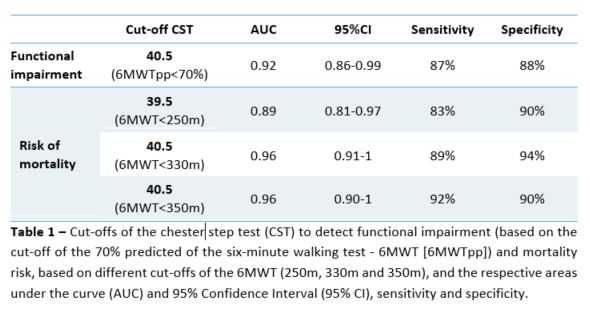
The 6MWT and CST were collected and a receiver operating characteristics (ROC) curve analysis was performed. We determined a threshold for the CST to detect: i) functional impairment, based on the 70% predicted of the 6MWT (6MWTpp<70%); and, ii) increased risk of mortality, based on different cut-offs of the 6MWT (250m, 330m and 350m). The optimal cut-off points were identified by the highest Youden index.
70 people with ILD (65 [57-75] years; 56% female; FVCpp 78.7±18.4; DLCOpp 53.7±19.7) were included. A cut-off of 40.5 steps was found to detect functional impairment (6MWTpp<70%) and increased risk of mortality (6MWT<330 and 350m). For those with <250m in the 6MWT a cut-off of 39.5 steps was found. The cut-off of 40.5 compared to 39.5 steps presented higher sensitivity (92% vs 83%) and equal specificity (90%) values (Table 1).
A cut-off of 40.5 steps in the CST may be used to detect functional impairment and/or at increased risk of mortality in people with ILD. This information may now be used to design tailored and preventive interventions, even in limited-space settings.