Abstract
The ability of pulmonary rehabilitation (PR) to modify physical activity (PA) of COPD patients remains controversial. We assessed the impact of PR on PA and explored PA change according to the response in other PR outcomes in COPD patients.
Exercise capacity (6MWT, 1minSTS), dyspnoea (mMRC), fatigue (FACIT-F), health-related quality of life (HRQoL, SGRQ), PA (steps/day and time spent in moderate to vigorous PA (MVPA)) were assessed before and after a 12-week PR program. Participants wore GT3X+ for 7 days (?4 valid days). Responders were defined based on MCID for the 6MWT (?25m), 1minSTS (?3reps), SGRQ (?-4points), FACIT-F (?5points), and mMRC (?-1point).
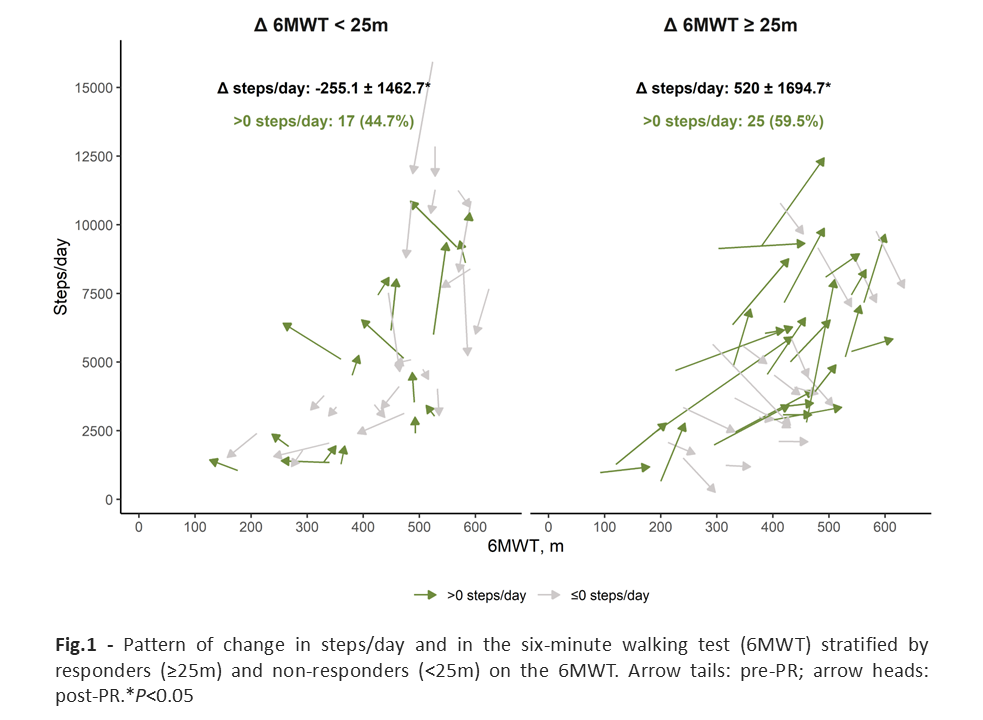
80 COPD patients (66% men; 70.2 ± 7.8y; FEV1 53.8 ± 15.6%p) were included. Improvements in exercise capacity (6MWT: 26.5 [-10, 55.73] and 1minSTS: 2.64 ± 4.84, P<0.01), HRQoL (-4.87 ± 10.56, P<0.01), dyspnoea (-0.5 [-1, 0], P<0.01) and fatigue (1.54 ± 6.24, P=0.03) were found. No change was observed in steps/day or MVPA neither between responders and non-responders in MVPA change. Only responders in the 6MWT improved significantly in steps/day (?25m: 519.95 ± 1694.71 vs <25m: -255.07 ± 1462.65; P=0.03, Cohen?s d=0.49). Nevertheless, change in steps/day within groups was highly heterogeneous (Fig.1).
PR does not seem to be sufficient to modify PA in COPD. Despite the small association with exercise capacity, PA change seems to be independent of the response in other PR outcomes.