Abstract
It is uncertain if pulmonary rehabilitation (PR) delivered in low-resource settings is as beneficial as in high-resource settings and can be consider to increase access. We compared the effects of PR delivered in low versus high-resource settings in people with chronic obstructive pulmonary disease (COPD).
12-week community-based PR programmes were conducted in one high (i.e., specialized centre) and five low-resource (i.e., primary care centres with limited equipment, facilities) settings. Symptoms (modified medical research council dyspnoea scale, functional assessment of chronic illness therapy?fatigue, hospital anxiety and depression scale), quadriceps maximum voluntary contraction, functional exercise capacity (6-minute walk test, 1-minute sit-to-stand test), balance (Brief-Balance Evaluation Systems Test) and health status (COPD assessment test) were assessed pre-post PR. Comparisons within and between groups were explored with (non-) parametric mixed ANOVAs.
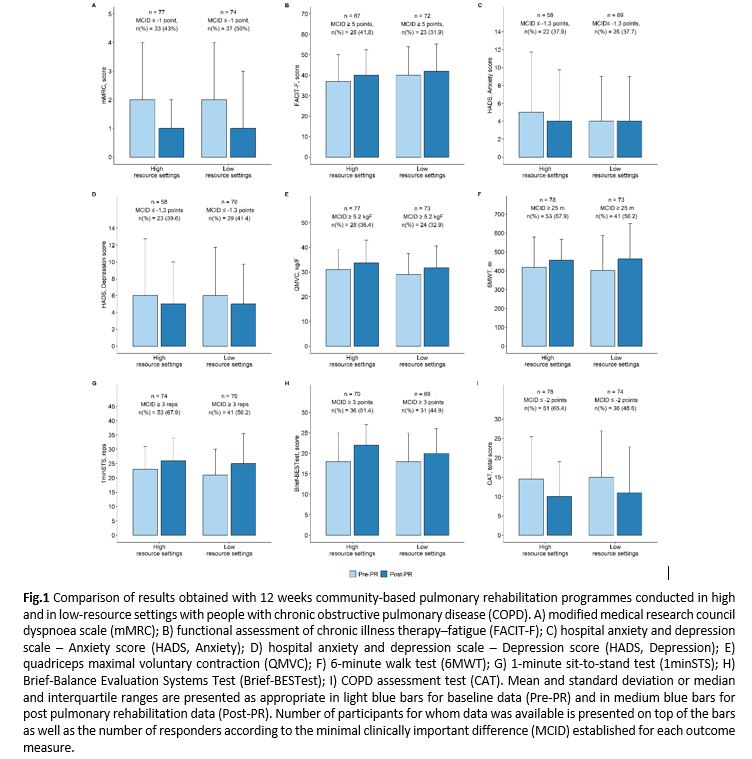
164 people with COPD (69±9yrs; 23% female; FEV1 53[38; 67]% predicted) participated, 83 in low- and 81 in high-resource settings. After PR, improvements were significant for all outcomes in both settings (p<0.05) (Fig.1). No group-by-time interaction or between-group differences were observed (p>0.05).
PR in low-resource settings provides similar benefits to high-resource settings and is important to be considered to increase access to this fundamental intervention.