Abstract
According to WHO Long COVID is defined as the continuation or development of new symptoms 3 months after the initial SARS-CoV-2 infection, with these symptoms lasting for at least 2 m with no other explanation and has a strong socioeconomic impact.We present the results of 49 pts (17man,32 women), 22 hospitalized, from LC patient Organization Greece with dyspnea and fatigue examined at the model interdisciplinary LC clinic of Evangelismos Hospital. LC pts that fulfilled WHO?s definition were examined according our proposed algorithm.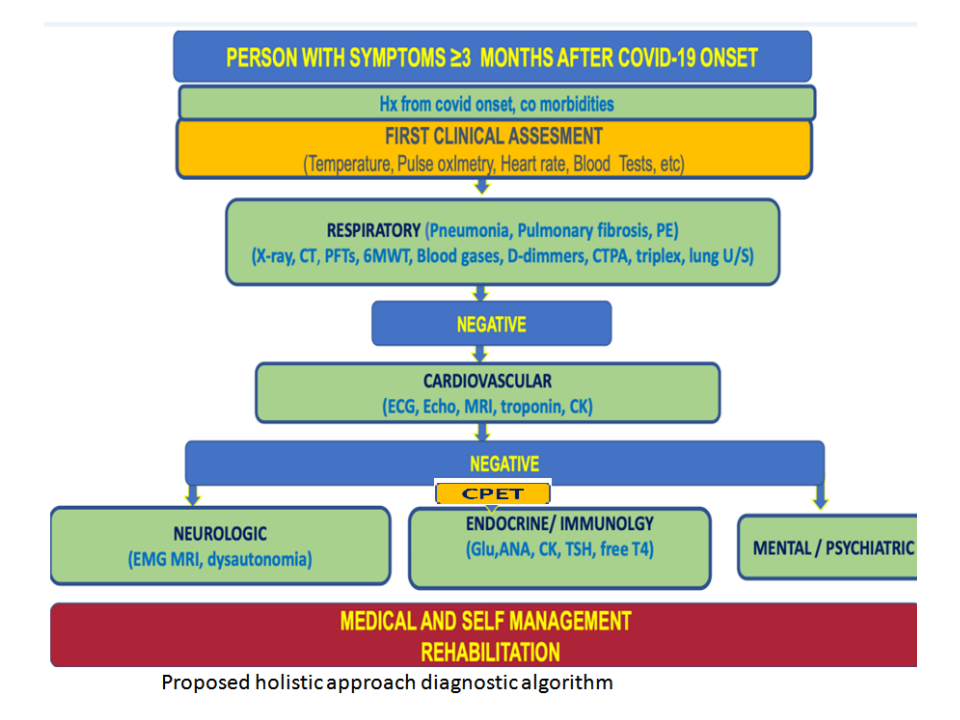 After examination form respiratory physicians and cardiologists, pts underwent ergospirometry test with 31(63.27%) of them showing abnormal results. Concretely, circulatory impairment was found in 18, abnormal ventilatory pattern in 18 neuromuscular problems in 6 and deconditioning in 12 pts. Interestinly, 23 LC pts (46,94%) were diagnosed with dysautonomia, with 17 of them having additionally impaired ergospirometry (9CVD involment, 5 respiratory, 4 neuromuscular) and decreased DLCO without pathologic findings in the CT scan. The involment of decreased DLCO without pathological findings in CT scan nor COPD diagnosis is fount in the majority of our pts (71,42%) and may be attributed to microvascular blood clotting with endothelial dysfunction. We believe that LC pts with shortness of breath and fatigue should indergo CPET, PFTs and neurologic examination in order to have a causal diagnosis with CPET having a key role.
After examination form respiratory physicians and cardiologists, pts underwent ergospirometry test with 31(63.27%) of them showing abnormal results. Concretely, circulatory impairment was found in 18, abnormal ventilatory pattern in 18 neuromuscular problems in 6 and deconditioning in 12 pts. Interestinly, 23 LC pts (46,94%) were diagnosed with dysautonomia, with 17 of them having additionally impaired ergospirometry (9CVD involment, 5 respiratory, 4 neuromuscular) and decreased DLCO without pathologic findings in the CT scan. The involment of decreased DLCO without pathological findings in CT scan nor COPD diagnosis is fount in the majority of our pts (71,42%) and may be attributed to microvascular blood clotting with endothelial dysfunction. We believe that LC pts with shortness of breath and fatigue should indergo CPET, PFTs and neurologic examination in order to have a causal diagnosis with CPET having a key role.