Abstract
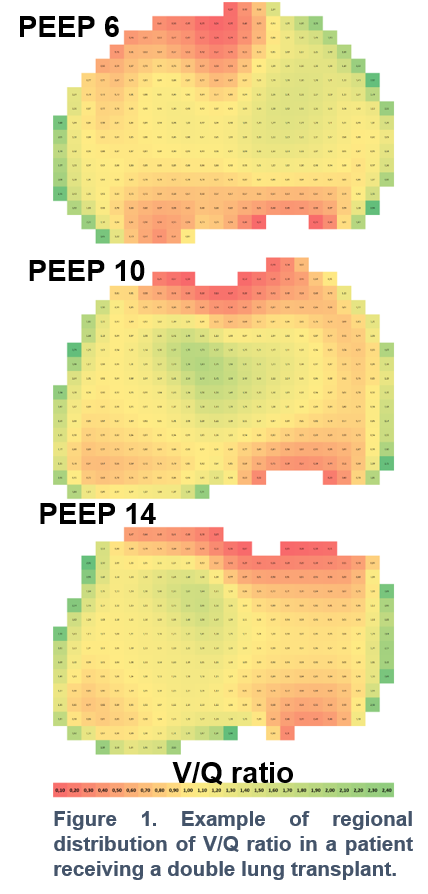
Management of mechanical ventilation and positive end-expiratory pressure (PEEP) selection after lung transplant (LUTX) is based on expert opinion. We obtained: 1/regional ventilation (V?)/perfusion (Q?) maps by integrating electrical impedance tomography (EIT), thermodilution technique, and volumetric capnometry; 2/ gas exchange; 3/ lung mechanics at 24 hours after reperfusion at 3 PEEPs (14, 10, and 6 cmH2O) in bilateral LUTX recipients protectively ventilated in volume control. To now, we enrolled 6 patients. EIT was feasible and - at all PEEP levels ? showed similar distributions of V? and Q? distribution between left and right grafts (and thus adequate functioning of bronchial or vascular anastomosis) but a wide variability in regional V?/Q? (Fig1).
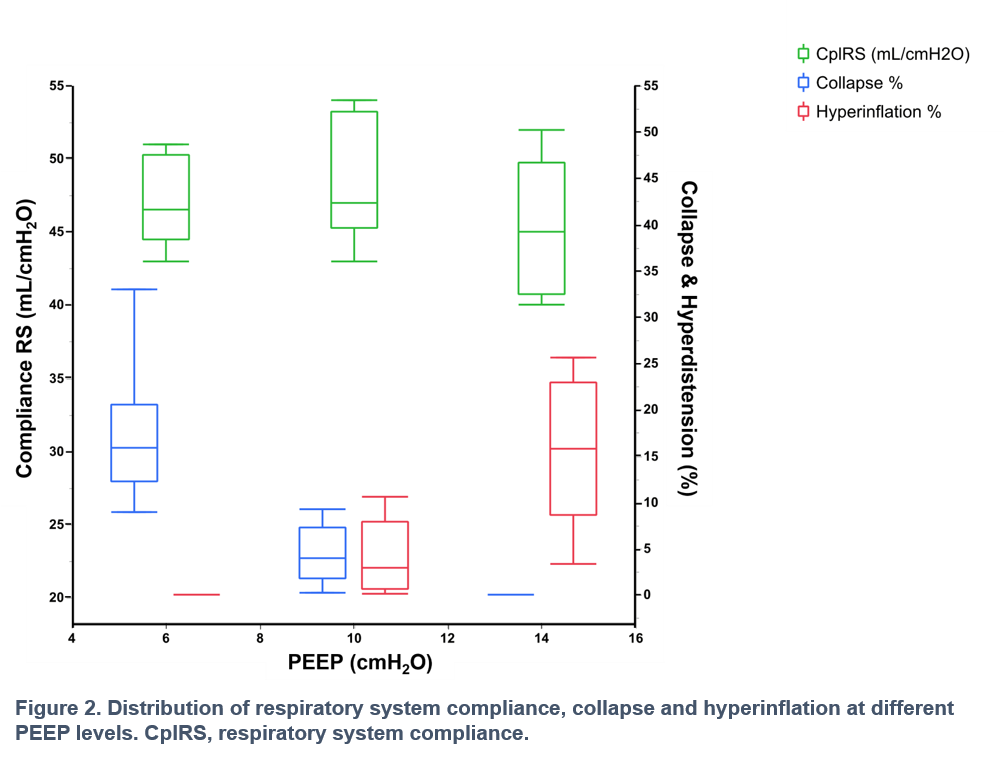
PEEP 10cmH2O resulted in the best respiratory system compliance and balance between collapse and hyperdistention (Fig2).
In the immediate post-LUTX period, EIT is a feasible bedside, non-invasive option to assess V? and Q? distribution. Since PEEP affects the regional V?/Q?, PEEP 10cmH2O might be a reasonable starting point to personalize ventilation.