Abstract
Background: Risk stratification in pulmonary arterial hypertension (PAH) relies on World Health Organisation Functional Class (WHO FC). A high proportion of patients are classified as WHO FC III with a resultant lack of nuance. The Medical Research Council (MRC) dyspnoea scale may allow a more precise assessment of functional status and improve current risk models.
Aim: Survival at baseline and follow up was retrospectively calculated using three models; the MRC dyspnoea scale, WHO FC and the COMPERA 2.0 model.
Methods: Patients with Idiopathic-, Hereditary- or Drug-induced PAH who were diagnosed between 2010 and 2021 were included. The MRC dyspnoea scale was retrospectively applied as derived from patient notes, 6MWD tests results and WHO functional status using a predefined algorithm. Survival was assessed using Kaplan-Meier analyses, logrank testing and Cox proportional hazards ratios.
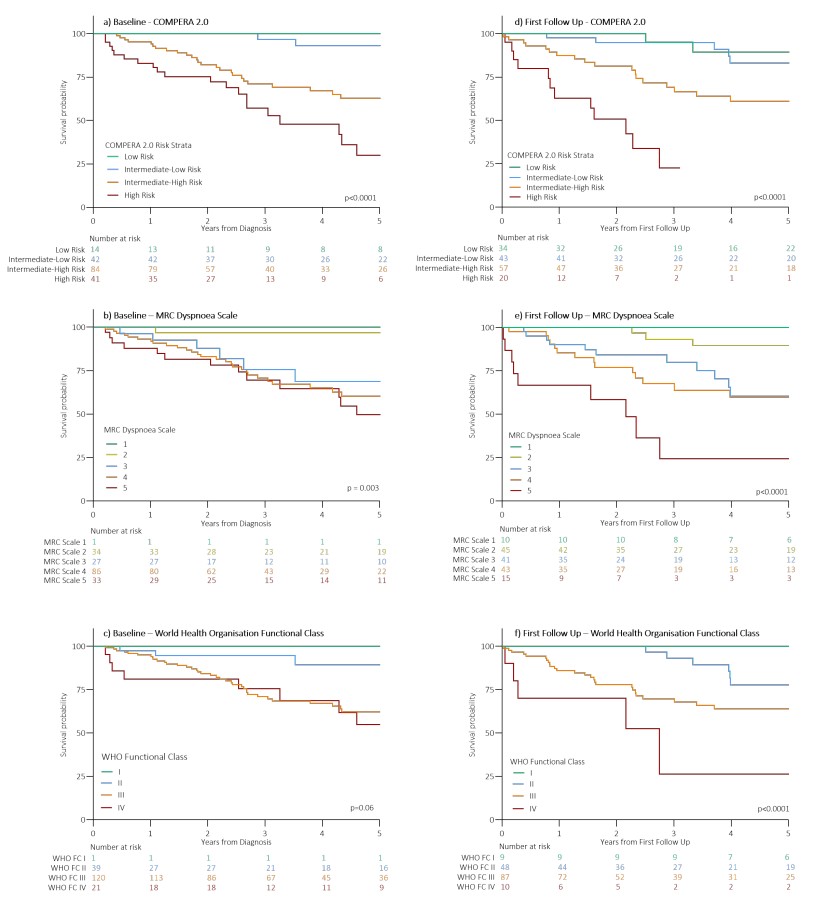
Results: Data from 216 patients were analysed. At baseline, of 120 patients classified as WHO FC III, 8% were MRC dyspnoea scale 2, 12% scale 3, 71% scale 4 and 10% scale 5. Between baseline and follow-up, 50% of patients changed risk category in the MRC dyspnoea model compared to 41% in the COMPERA 2.0 model and 33% for WHO FC. The MRC dyspnoea model performed well compared to other models (figure) with distinct hazard ratios.
Conclusion: At follow-up, the MRC dyspnoea scale proved more successful in assessing survival compared to WHO FC.