Abstract
Introduction: A network meta-analysis (NMA; Ismaila A.S. et al, Adv Ther 2022;39(11):4961?5010) compared the efficacy of UMEC/VI versus IND/GLY in symptomatic patients with COPD.
Aim and Objectives: To assess the cost-effectiveness of once-daily UMEC/VI 62.5/25µg versus once-daily IND/GLY 110/50µg for the treatment of COPD, from a United Kingdom (UK) National Healthcare System (NHS) perspective.
Methods: A validated linked risk equation model (GALAXY; Briggs A.H. et al, Med Decis Making 2017;37:4) which predicts COPD disease progression, healthcare costs, life-years (LYs) and quality-adjusted LYs (QALYs) was used. Baseline characteristics were derived from a clinical trial conducted in patients eligible for dual therapy (NCT02799784). Treatment effects were derived from an NMA and included change from baseline in FEV1, SGRQ, and reduction in exacerbations.
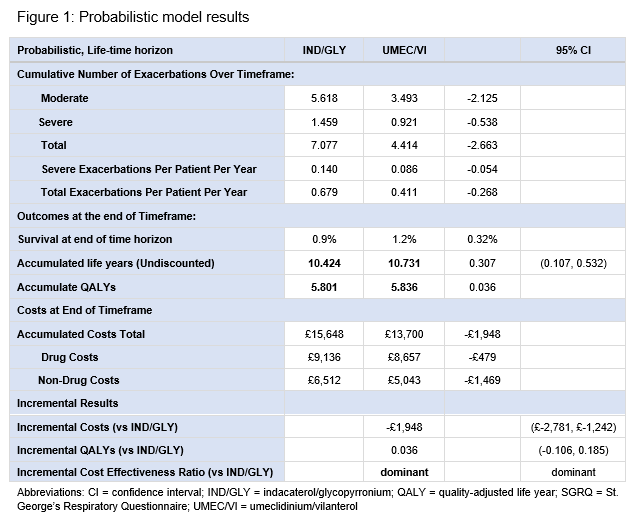
Results: Over a life-time horizon, UMEC/VI provided an additional 0.307 LYs and 0.036 QALYs, with cost savings of £1,948 versus IND/GLY. UMEC/VI was dominant versus IND/GLY across the majority of the scenarios and sensitivity analyses (exceptions include shorter time horizons, upper confidence interval for SGRQ and exacerbation treatment effects).
Conclusions: In a UK NHS setting, treatment with UMEC/VI was predicted to improve health outcomes and lower costs compared to IND/GLY in patients with symptomatic COPD.
Funding: GSK (217635)