Abstract
Introduction: Once-daily UMEC/VI 62.5/25µg was compared to twice-daily GLY/FOR 18/9.6µg in the AERISTO trial, a phase IIIb randomized, double-blind, 24-week study (Maltais F. et al, Adv Ther 2019;36[9]).
Aim and Objectives: To assess cost-effectiveness of UMEC/VI vs GLY/FOR for treatment of symptomatic patients with COPD from a UK National Healthcare System perspective using AERISTO data.
Methods: Analysis conducted using a validated model implemented using a linked risk-equation approach (GALAXY; Briggs A.H. et al, Med Decis Making 2017;37:4) to model disease progression and predict healthcare costs, life-years (LYs) and quality-adjusted LY (QALYs). Baseline characteristics and treatment effects (change in FEV1 and in SGRQ [derived from exploratory CAT score mapping]) were derived from the AERISTO trial.
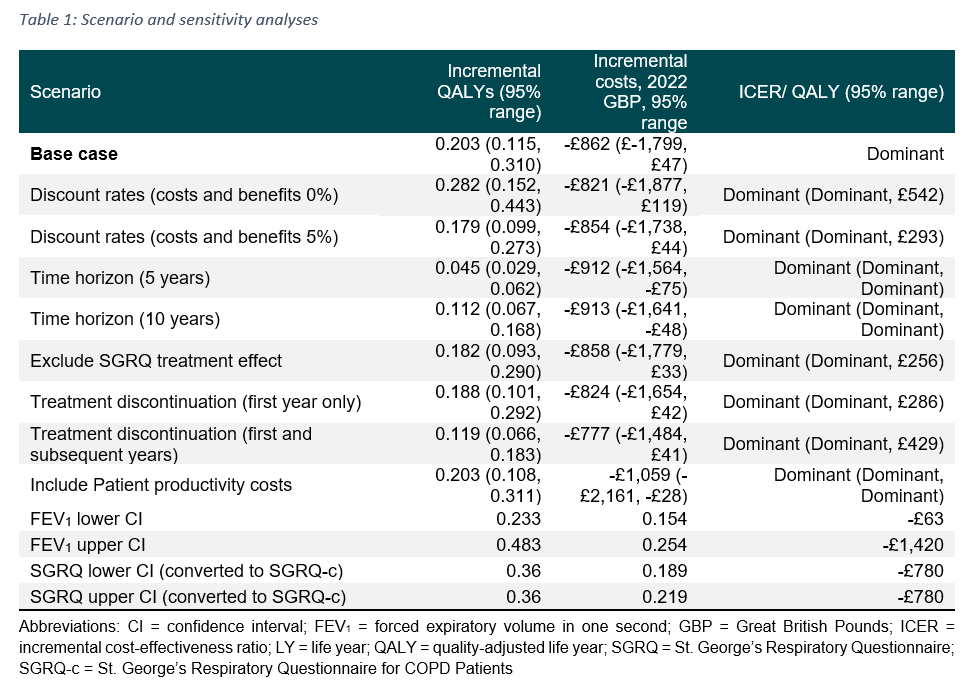
Results: Over a life-time horizon, compared to GLY/FOR, UMEC/VI provided fewer number of exacerbations (0.116), and additional LYs (0.354; 95% range 0.158, 0.592) and QALYs (0.203; 95% range 0.115, 0.310), with cost savings of £862 (95% range -£1,799, -£47). Scenario and sensitivity analyses showed consistently similar results.
Conclusions: UMEC/VI is estimated to reduce the overall economic burden of COPD and should be considered by physicians as a preferred treatment option for symptomatic patients with COPD in the UK.
Funding: GSK (217635)