Abstract
Introduction:Large airway collapse(LAC) is a prevalent but often overlooked cause of complex breathlessness and refractory airway symptoms. The diagnostic criteria for LAC remain unclear and a variety of protocols are proposed. We compare likelihoods of detecting LAC on CT imaging dependent on the imaging acquisition protocol employed.
Method:We retrospectively reviewed reports of CT scans performed to detect LAC over a 12-month period in a specialist severe asthma service by means of 2 CT manoeuvres; Dynamic(DE) and Forced Expiration(FE). Large airway collapse was defined as >/=70% reduction in cross sectional area at the trachea +/- main bronchi on expiration compared with end inspiration. Those who did not complete both expiratory CT manoeuvres and reports without indication of degree of collapse in % were excluded.
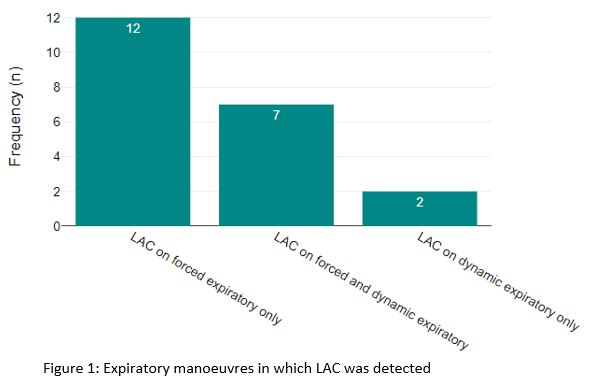
Result:21 patients (n=19 female) out of a total of 105 undergoing CT were found to have LAC, with a mean age of 54.2±12.0 years and a mean BMI of 40.4± 6.8kg/m2 were found to have LAC. Of these, LAC was observed on both FE and DE in 7 cases, on FE only in 12 cases, and on DE only in 2 cases. Large airway collapse was detected in a significantly greater proportion of patients with FE 19(90%) than with DE 9(43%) (McNemar?s chi-square test, p=0.01).
Conclusion:The inclusion of a forced expiratory protocol is associated with improved detection of LAC in patients referred with refractory airways disease.