Abstract
Aim: MRI ventilation defects in acute asthma are not homogeneous. We assessed topographical ventilation differences following direct (methacholine (MCh)) and indirect (mannitol) inhalational challenges in mild asthma to improve our understanding of their pathophysiology.
Methods: Asthmatic subjects underwent spirometry and hyperpolarised helium MRI (He3MRI) ventilation scans pre and post inhalation of either MCh or mannitol (at their known provocative concentration/dose), with repeat scans using alternate challenge test on a separate day. He3MRI ventilation was quantified using k-means segmentation.
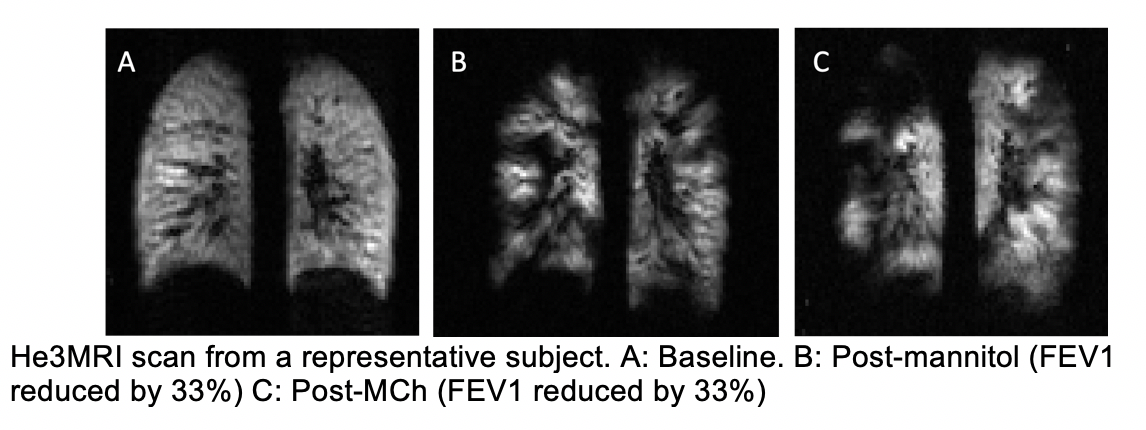
Results: 8 subjects were studied. Mean age was 35.9±9.8 years and 75% were females. Baseline FEV1 was 95.3±12.8% and fell by 24±7% post MCh. Post mannitol, FEV1 fell by 18±11% from a baseline of 94.0±12.4%. Ventilation abnormalities seen at baseline were worse post-challenge. Regions of poor ventilation also increased from 10.3% to 17.8% with MCh and from 11.9% to 15.1% with mannitol. Overlap between regions affected by either challenge test was also noted.
Conclusion: Direct and indirect airway challenges have different topographical distributions in ventilation defects despite a similar fall in FEV1. Certain airways also appear to be more susceptible to bronchial provocation regardless of the challenge method. This reinforces the notion that asthma is a heterogeneous disease.