Abstract
Background: Recent data indicate methamphetamine pulmonary hypertension (meth-PAH) has higher mortality and worse right ventricular (RV) function than idiopathic PAH (iPAH) although meth-PAH is less often treated with parenteral prostacyclin. Our study aims to evaluate mortality and RV function in these groups treated with subcutaneous treprostinil (TRE).
Methods:
The analysis included incident functional class IIIB-IV iPAH and meth-PAH subjects eligible for parenteral prostacyclin based on guidelines. RV function was assessed with tricuspid annular plane systolic excursion (TAPSE)/systolic pulmonary artery pressure (sPAP). Survival analysis was assessed using Kaplan-Meier and log rank test.
Results:
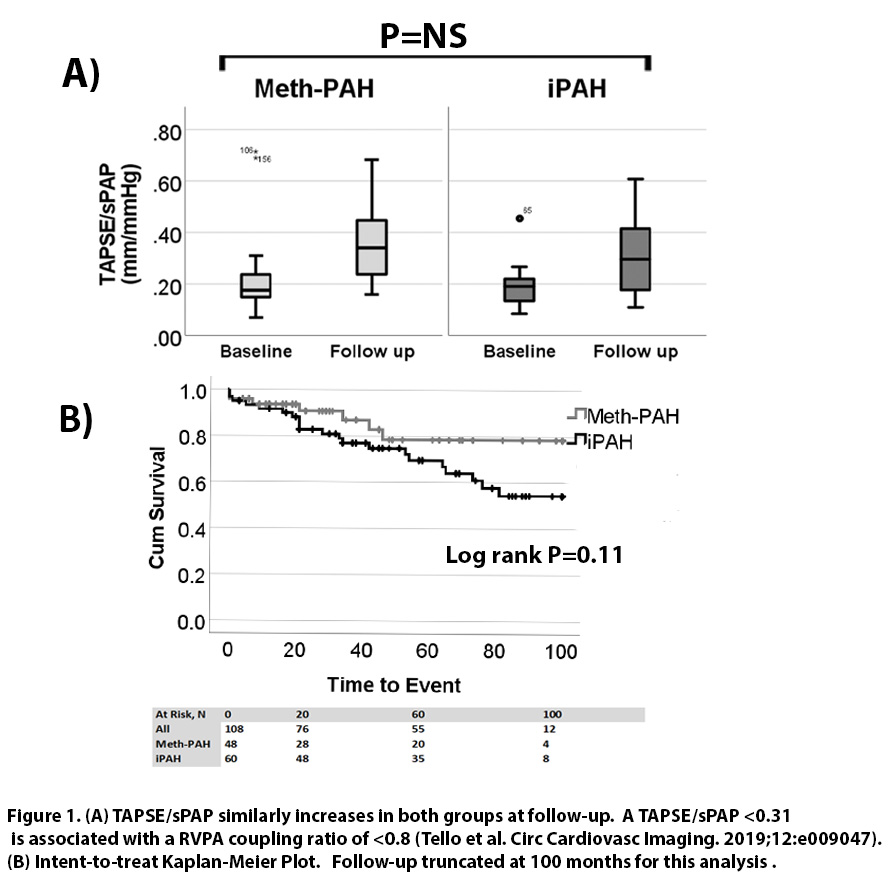
The analysis included 48 meth-PAH and 60 iPAH incident functional class III-IV patients. 8 meth-PAH (17%) versus 3 (3%) iPAH did not start TRE (despite the indication) due to safety concerns. 1 (3%) meth-PAH and 3 (5%) iPAH patients were transitioned off TRE due to adverse events over a mean follow up of 53 months [range 0-155]. There were no baseline or treatment related differences in sex, age, pulmonary vascular resistance, right atrial pressure, or RV function (Figure 1A). Mortality was similar early in follow up but cumulatively lower in meth-PAH subjects (8, 17% versus 21, 38%) (Figure 1B).
Conclusions: When treated alike per guidelines, meth-PAH patients have similar safety and treatment response to iPAH.