Abstract
Rationale: Physicians often wait for progression to initiate or escalate therapy in SSc-ILD assuming that patients with recent ILD progression have a higher risk for further progression.
Objective: Assess whether ILD progression predicts subsequent progression.
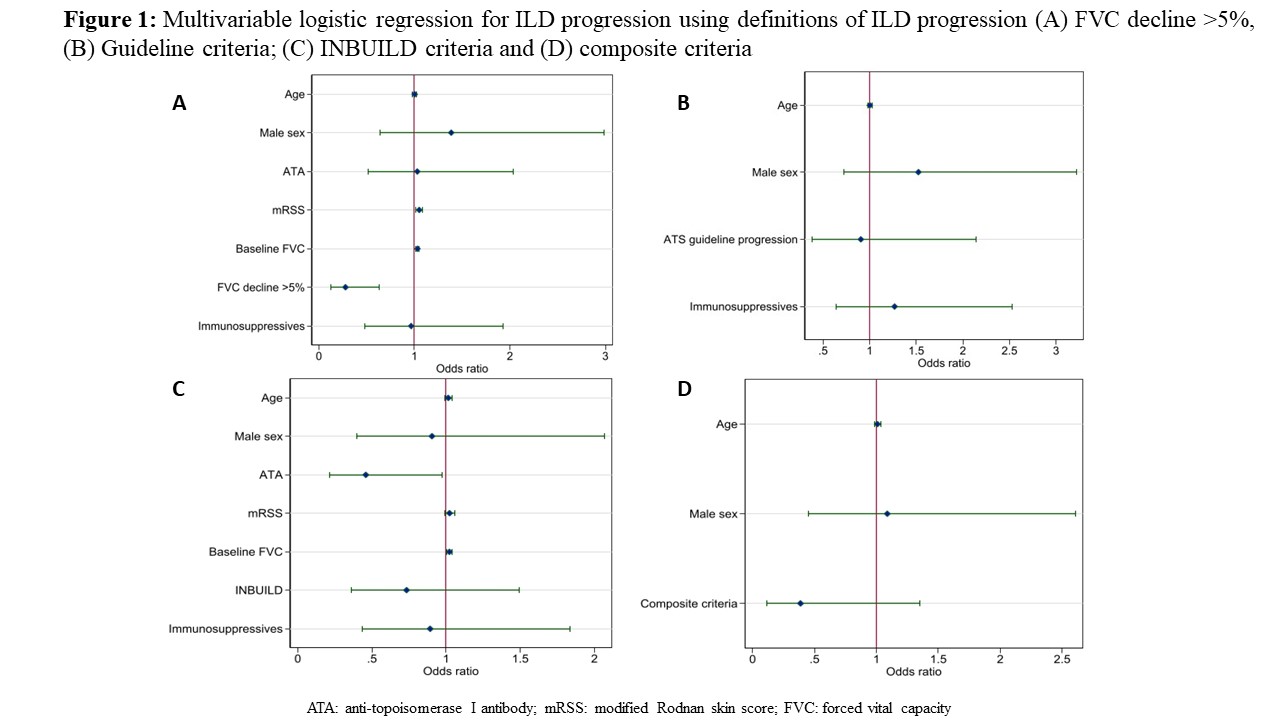
Methods: We included all SSc-ILD patients from the Oslo and Zurich cohorts with serial FVC. ILD progression was defined as absolute FVC decline >5%. At follow up, we again assessed progression. We applied other definitions: (A) 2022 Guideline criteria (PPF); (B) INBUILD (PF-ILF); (C) Composite criteria (absolute FVC ?10%; or FVC >5%-9% and DLCO >15% decline). Multivariable logistic regression adjusted for known risk factors and treatment was applied.
Results: Here, 231 SSc-ILD patients including 24% males, 41% with diffuse cutaneous SSc were assessed. At 12 months, 31% showed FVC decline >5%. In multivariable logistic regression, ILD progression was significantly protective for further progression at follow up (OR 0.28, 95%CI 0.12-0.63, p=0.002, Figure1a). Results for PPF, PF-ILD and for composite decline showed the same directions (Figure1b-d).
Conclusion: ILD progression does not predict further progression using any ILD progression definition in SSc. This has important implications for clinical practice and clinical trial design.