Abstract
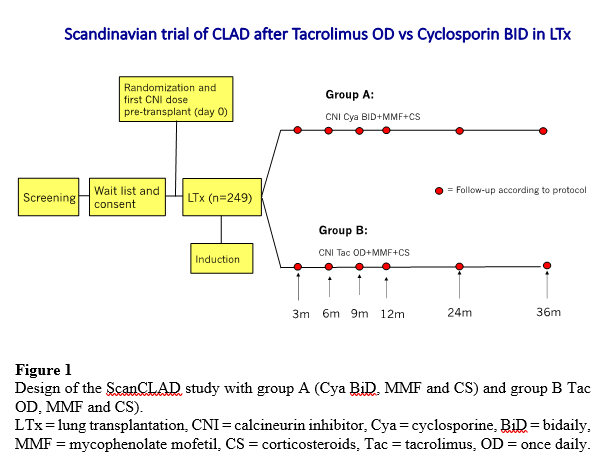
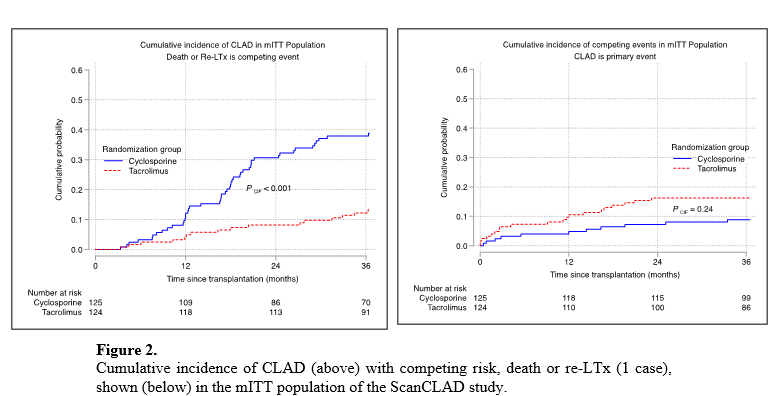
Background: Evidence is low regarding the choice of calcineurin inhibitor (CNI) for immunosuppression after lung transplantation (LTx). No other randomized controlled trial (RCT) has compared tacrolimus (Tac) once daily with cyclosporine (Cya) twice daily according to the current definition of chronic lung allograft dysfunction (CLAD) after LTx. Methods: ScanCLAD is an investigator-initiated, open-label, multi-center RCT evaluating if an immunosuppressive protocol based on ATG-induction, once daily Tac-dose, mycophenolate mofetil and corticosteroid, reduces the incidence of CLAD after de novo LTx, compared to a Cya-based protocol. Patients (n=249, age 18-70) underwent double LTx with three-year follow-up. Primary endpoint CLAD was determined by repeated lung function tests and adjudicated by an independent committee. The diagnosis of acute rejection (AR) was based on clinical signs or histological biopsy confirmation. Findings: The cumulative incidence of the primary endpoint, CLAD at 36 months post-transplant, was significantly higher in the Cya-group (48/119 (40·3%) versus Tac: 16/115 (13·9%); (HR 0·28 (95%CI 0·15-0·52); p<0·001, log-rank)(Figure 1). The composite measure of event-free survival from treated AR, CLAD, graft loss, or patient death respectively at 12, 24 and 36 months after transplantation was significantly worse for Cya (45% (95%CI 36-54), 32% (95%CI 24-41), 28% (95%CI 20-37)) compared to Tac (57% (95%CI 48-66), 55% (95%CI 45-63), 52% (95%CI 42-61), HR 0·59 (95%CI 0·42-0·83); p<0·002, log-rank)(Figure 2). Overall survival did not differ between groups at three years in the mITT population (Cya: 74% (95%CI 65-81) and Tac: 79% (95%CI 70-85), HR 0·72 (95%CI 0·41-1·27); p=0·25, log-rank). However, in the per protocol CLAD population allograft survival was significantly better in the Tac group (HR 0·49 (95%CI 0·26-0·91); p=0·021, log-rank). The Hazard Ratio for CLAD in between groups was 0·27 (95%CI 0·15-0·52) and NNT was 3·8 (95%CI 3·3-4·4) to prevent one CLAD by using Tac. Interpretation: Tac-based immunosuppression once daily significantly reduced the incidence of CLAD compared to Cya twice daily, and Tac should be regarded as first CNI choice after LTx. Further, the Tac group had significantly higher event-free survival when combining treated AR, CLAD, graft loss and patient death, and allograft survival was significantly better in the CLAD per protocol population.