Abstract
Introduction: Most evidence underpinning pulmonary rehabilitation (PR) comes from RCTs using specialist exercise equipment (PR-specialist). PR programmes using minimal equipment (PR-min) are more accessible alternatives, but efficacy compared with PR-specialist remains uncertain.
Aim: To determine if centre-based PR-min is non-inferior to PR-specialist for the effect on exercise capacity in chronic lung disease.
Methods: Parallel, two-group, non-inferiority RCT. Adults with stable chronic respiratory disease were allocated (1:1) to PR-min or PR-specialist, with matched supervision, staffing and training frequency. The primary outcome, change in incremental shuttle walk (ISW) distance from baseline to 8 weeks, was compared on an intention to treat basis using a one-sided t-test (sig level p=0.025). The non-inferiority margin was set at -24m.
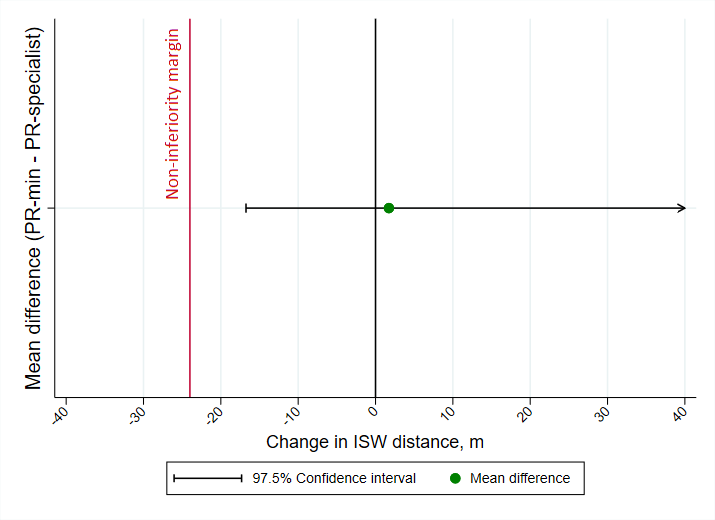
Results: 436 patients: mean(SD) age 70(11), 55% male, 63% COPD, were randomised. 74 were unable to receive PR due to Covid-19 disruptions. Baseline ISW distances were 274.0(171.8)m PR-specialist and 297.4 (190.0)m PR-min. Paired data (n=266) showed mean [95%CI] changes of 23.0 [11.9-34.2]m and 24.7 [10.0-39.5]m respectively. The mean difference in primary outcome was 1.7m and the lower 97.5%CI of -16.8m did not cross the non-inferiority margin (p=0.0034, Figure).
Conclusion: PR-min is non-inferior to PR-specialist for its effect on exercise capacity in chronic lung disease.