Abstract
Objectives
Investigate the influence of fever duration on the diagnostic performance of readily available blood biomarkers for community-acquired pneumonia (CAP) in children.
Study Design
We retrospectively analyzed 3346 children (2-18) with physician-diagnosed CAP at a teritary hospital ER, excluding those with major comorbidities or missing data (fever duration, biomarkers, chest X-rays). Optimal biomarker cutoffs were identified. AUC assessed biomarker performance for differentiating radiological definite CAP from LRTI symptoms.
Of the 509 children meeting inclusion criteria (363 definite CAP),Neutrophil-Lymphocyte Ratio (NLR)(cutoff 4.5) displayed significant discriminatory power from days 2-5, peaking on day 4 with AUC 0.70 (95% CI: 0.54-0.86). WBC (15,000/mm³) and ANC (11,200/mm³) peaked on day 2, while CRP (6.23 mg/dl) peaked on day 4 with AUC 0.81 (95% CI: 0.67-0.95). None reliably diagnosed CAP on day 1.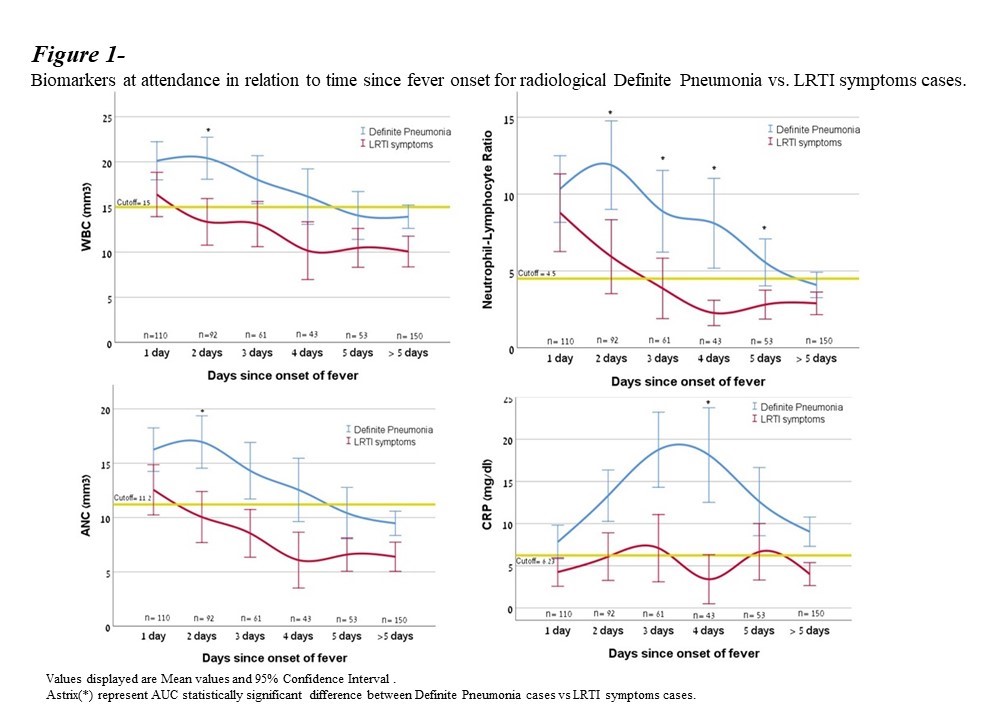
Conclusions
This study underscores the time-dependent nature of biomarker performance in pediatric CAP. While no biomarker reliably diagnosed CAP on day 1, NLR demonstrated consistent reliability across multiple days, peaking on day 4. These findings support its potential for clinical decision-making and highlight the importance of considering fever duration for optimal diagnostic accuracy.